This is a sensitive topic – Sweeteners (Natural and Artificial)

Lets start with the primary question.
Is it possible to eat sweets when you have diabetes?
The answer is “yes.” But when you’re trying to satisfy your sweet tooth, it can be hard to know what to reach for at the grocery store (sugar-free this or low-calorie that). So, use this primer to help you choose wisely.
The Sweet Facts
When you’re comparing sweeteners, keep these things in mind:
- Sugars are naturally occurring carbohydrates. These include brown sugar, cane sugar, confectioners’ sugar, fructose, honey, and molasses. They have calories and raise your blood glucose levels (the level of sugar in your blood).
- Reduced-calorie sweeteners are sugar alcohols. You might know these by names like isomalt, maltitol, mannitol, sorbitol, and xylitol. You’ll often find them in sugar-free candy and gum. They have about half the calories of sugars and can raise your blood sugar levels, although not as much as other carbohydrates.
- Artificial sweeteners are considered “free foods.” They were designed in a lab, have no calories, and do not raise your blood sugar levels.
Types of Artificial Sweeteners
Artificial low-calorie sweeteners include:
- Saccharin (Sweet’N Low, Sugar Twin). You can use it in both hot and cold foods. Avoid this sweetener if you are pregnant or breastfeeding.
- Aspartame (NutraSweet, Equal). You can use it in both cold and warm foods. It may lose some sweetness at high temperatures. People who have a condition called phenylketonuria should avoid this sweetener.
- Acesulfame potassium or ace-K (Sweet One, Swiss Sweet, Sunett). You can use it in both cold and hot foods, including in baking and cooking.
- Sucralose (Splenda). You can use it in hot and cold foods, including in baking and cooking. Processed foods often contain it.
- Advantame can be used in baked goods, soft drinks and other non-alcoholic beverages, chewing gum, candies, frostings, frozen desserts, gelatins and puddings, jams and jellies, processed fruits and fruit juices, toppings and syrups.
Read Between the Lines
Use this “cheat sheet” to identify which products are sweetened the way you want them.
- No sugar or sugar-free. The product does not contain sugar at all, though it may contain sugar alcohols or artificial sweeteners.
- No added sugar. During processing, no extra sugar was added. However, the original source might have contained sugar, such as fructose in fruit juice. Additional sweeteners such as sugar alcohols or artificial sweeteners also might have been added.
- Dietetic. The product may have reduced calories, but this word can mean a lot of things.
When in Doubt, Read the Nutrition Label
To know for sure what kind of sweetener a food product contains, check the Nutrition Facts label. In the Carbohydrate section, you can see how many carbohydrates the product has, and how much of these carbohydrates are in the form of sugar or sugar alcohol.
For even more nutrition information, read the Ingredients list. It should show any added sweeteners, whether they are sugars, sugar alcohols, or artificial.
By understanding more about artificial sweeteners and diabetes, you will be able to make better food choices as you balance sweetness with good blood sugar control.
What are artificial sweeteners? Comparison
Artificial sweeteners can be used instead of sugar to sweeten foods and drinks. You can add them to drinks like coffee or iced tea, and they are found in many foods sold in grocery stores. These sweeteners, also called sugar substitutes, are made from chemicals and natural substances.
Sugar substitutes have very few calories compared to sugar. Some have no calories. Many people use sugar substitutes as a way to limit how much sugar they eat, whether it’s to lose weight, control blood sugar, or avoid getting cavities in their teeth.
If your goal is to lose weight, keep in mind that even though a food is sugar-free, it can still have carbohydrates, fats, and calories. It’s a good idea to read the nutrition label to check for calories and carbohydrate. Sugar alcohols are also used to sweeten diet foods and drinks. These plant-based products include mannitol, sorbitol, and xylitol. If you eat too much of them, sugar alcohols can cause diarrhea, bloating, and weight gain.
Are sugar substitutes safe?
Yes. The FDA regulates the use of artificial sweeteners. At one time, saccharin was thought to increase the risk of bladder cancer in test animals. Studies reviewed by the FDA have found no clear evidence of a link between saccharin and cancer in humans.
People who have phenylketonuria (PKU) should avoid foods and drinks that have aspartame, which contains phenylalanine.
Do artificial sweeteners raise blood sugar?
No. Artificial sweeteners provide no energy, so they won’t affect your blood sugar. If you have diabetes, these substitutes are safe to use. But that’s not true of sugar alcohols. They don’t cause sudden spikes in blood sugar, but the carbohydrate in them can affect your blood sugar.
If you have diabetes, read food labels carefully to find out the amount of carbohydrate in each serving of food containing sugar alcohol. It’s also a good idea to test your blood sugar after you eat foods with sugar alcohols or artificial sweeteners to find out how they affect your blood sugar.
How do sugar substitutes compare?
| Sweetener name |
Can be used for cooking and baking |
| Aspartame (NutraSweet, Equal) |
No, because it breaks down during cooking |
| Saccharin (Sweet’N Low) |
Yes |
| Sucralose (Splenda) |
Yes |
| Acesulfame K (Sunett) |
Yes |
| Stevia (Truvia, PureVia, SweetLeaf) |
Yes |
Diet foods and drinks are promoted to help you lose weight but compelling evidence shows that artificial sweeteners like aspartame cause weight gain rather than weight loss. That’s right, aspartame―which was once hailed as a wonder chemical because it tastes like sugar without the calories―actually makes you fatter, and adversely affects your blood glucose levels and insulin sensitivity.
So far so good – right? – Well, there are controversies & for the sake of information, read on. Studies Repeatedly Find Aspartame Causes Weight Gain
 The fact that aspartame is NOT a dieter’s best friend has been known by scientists for some time. The problem is this news has not received the necessary traction in the media. For example, a study from 19861, which included nearly 80,000 women, found that those who used artificial sweeteners were significantly more likely than non-users to gain weight over time, regardless of initial weight. According to the authors, the results “were not explicable by differences in food consumption patterns,” and concluded that:“ The data do not support the hypothesis that long-term artificial sweetener use either helps weight loss or prevents weight gain.”
The fact that aspartame is NOT a dieter’s best friend has been known by scientists for some time. The problem is this news has not received the necessary traction in the media. For example, a study from 19861, which included nearly 80,000 women, found that those who used artificial sweeteners were significantly more likely than non-users to gain weight over time, regardless of initial weight. According to the authors, the results “were not explicable by differences in food consumption patterns,” and concluded that:“ The data do not support the hypothesis that long-term artificial sweetener use either helps weight loss or prevents weight gain.”
Another more recent study with the telling title of Gain Weight by “Going Diet?” Artificial Sweeteners and the Neurobiology of Sugar Cravings, published in 2010, found that epidemiologic data suggest artificially sweetened foods and beverages do not reduce weight.
Quite the contrary: “Several large scale prospective cohort studies found positive correlation between artificial sweetener use and weight gain. The San Antonio Heart Study examined 3,682 adults over a seven- to eight-year period in the 1980s. When matched for initial body mass index (BMI), gender, ethnicity, and diet, drinkers of artificially sweetened beverages consistently had higher BMIs at the follow-up, with dose dependence on the amount of consumption… Saccharin use was also associated with eight-year weight gain in 31,940 women from the Nurses’ Health Study conducted in the 1970s.
Similar observations have been reported in children. A two-year prospective study involving 166 school children found that increased diet soda consumption was associated with higher BMI Z-scores at follow-up, indicating weight gain. The Growing Up Today Study, involving 11,654 children aged 9 to 14, also reported positive association between diet soda and weight gain for boys. For each daily serving of diet beverage, BMI increased by 0.16 kg/m2… A cross-sectional study looking at 3,111 children and youth found diet soda drinkers had significantly elevated BMI.”
Study Finds Aspartame Worsens Insulin Sensitivity
A recent study published in PLoS One found that chronic lifetime exposure to aspartame, commencing in utero, produces changes in blood glucose parameters and adversely impacts spatial learning and memory in mice. The study, which was published, was a blow against claims that aspartame is an ideal sugar substitute for diabetics.
The researchers used a dosage of aspartame that approximates the ADI for aspartame in the US (approx. 50 mg/kg body weight), and not only was aspartame found to decrease insulin sensitivity compared to controls, it also wrought havoc on brain function.As mentioned on countless occasions, optimizing your insulin sensitivity is key for optimal health, as insulin resistance is a hallmark of virtually every chronic disease you can think of, but especially type 2 diabetes.
Now, contrary to popular belief, aspartame is being revealed as a substance that actually decreases or worsens insulin sensitivity, which is the complete opposite of what you want—especially if you’re already pre-diabetic or diabetic!
According to the authors:“At 17 weeks of age, male aspartame-fed mice exhibited weight gain, elevated fasting glucose levels and decreased insulin sensitivity compared to controls. Females were less affected, but had significantly raised fasting glucose levels.During spatial learning trials in the MWM (acquisition training), the escape latencies of male aspartame-fed mice were consistently higher than controls, indicative of learning impairment… Interestingly, the extent of visceral fat deposition correlated positively with non-spatial search strategies such as floating and thigmotaxis, and negatively with time spent in the target quadrant and swimming across the location of the escape platform.
These data suggest that lifetime exposure to aspartame, commencing in utero, may affect spatial cognition and glucose homeostasis in C57BL/6J mice, particularly in males.”
Male mice fed aspartame experienced significantly higher weight gain compared to the control group, whereas female weight gain was unaffected by the aspartame diet compared to controls. However, deposits of visceral fat—those dangerous fat deposits around internal organs, which are associated with an increased risk of heart disease in humans—increased in aspartame-fed mice of both sexes. Aspartame-fed mice of both sexes also had elevated fasting blood glucose levels compared to non-consumers of aspartame, although the male mice experienced higher elevations than the females.According to the authors:
Surprise: Aspartame raises insulin levels as much as sugar
Another study published in 2007 in the journal Diabetes Care found similar results. Here, the researchers investigated the effect of different macronutrient compositions on plasma glucose and insulin levels during an acute bout of exercise in men with type 2 diabetes. They compared the subjects in five different conditions:
- high–glycemic index sucrose meal (455 kcal)
- low–glycemic index fructose meal (455 kcal)
- aspartame meal (358 kcal)
- high-fat/low-carbohydrate meal (455 kcal)
- fasting
They hypothesized that using fructose or aspartame would have a lower impact on insulin release and glucose response than a sucrose-sweetened meal. However, experts on sugar and fructose like Dr. Richard Johnson and Dr. Robert Lustig will immediately recognize this as a fatally flawed hypothesis. And indeed, that is what they discovered as well.
According to the authors:“Contrary to all expectation, the aspartame breakfast induced a similar rise in glucose and insulin levels at baseline than the sucrose meal, even if the aspartame meal had the same taste, and was 22 percent lower in calories and 10 percent lower in carbohydrates, with an inferior glycemic index.… Considering the lack of evidence on the aspartame utilization in patients with type 2 diabetes, we consider that these clinical observations, in an exercise setting, raise important concerns regarding the safety of aspartame as suggested by international guidelines.”
European Food Safety Authority to Re-Evaluate Aspartame
In related news, the European Commission (EC) has asked the European Food Safety Authority (EFSA) to speed up the full re-evaluation of aspartame (approved in Europe under the designation E951). Previously planned to be re-evaluated by 2020, the EC is now asking for the review of aspartame to be initiated this year.
According to a notice by EFSA:“In the course of its scientific deliberations, the Panel found that there were too little data available on 5-benzyl-3, 6-dioxo-2-piperazine acetic acid (DKP) and other potential degradation products that can be formed from aspartame in food and beverages when stored under certain conditions. EFSA is therefore launching an additional call for data on DKP and other degradation products of aspartame.”
Aspartame’s three components are phenylalanine (50 percent), aspartic acid (40 percent), and methanol (10 percent). When aspartame is exposed to heat or prolonged storage, it breaks down into metabolites. One of these breakdown products is Diketopiperazine (DKP), a toxic metabolite that is not usually found in our diet. The effects of these different metabolites are unknown. It will be interesting to see what, if anything, the EFSA re-evaluation will find out about these metabolites, but regardless, it stands to reason that anything not normally found in actual food is probably not suitable to eat if you’re interested in maintaining optimal health… After all, the human body is designed to run on nutrients, not foreign chemicals.
Retraining Your Taste Buds is Necessary if You Want Good Health
The idea that you can have your sweets without paying the price of excess weight and related health problems is a persistent one, but it’s not one we’re likely to solve anytime soon. Still, beverage manufacturers like PepsiCo and Coca-Cola are hard at work searching for the magic ingredient that will quench your thirst for sugary sweetness without the extra calories.
As reported by SeattlePi.com, increasing awareness of the harmful effects of both high fructose corn syrup and artificial sweeteners has soda makers searching high and low for new naturally occurring sweeteners. Some extracts currently under consideration include stevia, monk fruit, and miracle fruit.
Whether or not any of them will actually be able to let you have your soda without suffering negative consequences remains to be seen. But one thing is for certain, and that is that artificial sweeteners have completely failed in this regard. The evidence showing that artificial sweeteners actually worsen the conditions it’s supposed to ameliorate—primarily obesity and diabetes—is quite overwhelming, and since its approval aspartame has been linked to all sorts of health problems.
The following chronic illnesses can be triggered or worsened by ingesting of aspartame:
- Brain tumors
- Multiple Sclerosis
- Epilepsy
- Chronic Fatigue Syndrome
- Parkinson’s Disease
- Alzheimer’s
- Lymphoma
- Diabetes
Aspartame and MSG Implicated in Worsening Fibromyalgia and Irritable Bowel Symptoms
Another recent study published in the journal Clinical and Experimental Rheumatologyreveals a potential link between aspartame and conditions such as fibromyalgia and irritable bowel syndrome (IBS).
Both monosodium glutamate (MSG) and aspartate—one of the main ingredients in aspartame—are considered “excitotoxic,” meaning they can excite brain neurons to the point of death.According to the authors:“Fifty-seven fibromyalgia patients who also had irritable bowel syndrome (IBS) were placed on a 4-week diet that excluded dietary additive excitotoxins including MSG and aspartame. Thirty-seven people completed the diet and 84 percent of those reported that >30% of their symptoms resolved, thus making them eligible to proceed to challenges.
Subjects who improved on the diet were then randomised to a 2-week double-blind placebo-controlled crossover challenge with MSG or placebo for 3 consecutive days each week.… The MSG challenge, as compared to placebo, resulted in a significant return of symptoms; a worsening of fibromyalgia severity… decreased quality of life in regards to IBS symptoms… and a non-significant trend toward worsening fibromyalgia pain based on visual analogue scale.
These findings suggest that dietary glutamate may be contributing to fibromyalgia symptoms in some patients. Future research on the role of dietary excitotoxins in fibromyalgia is warranted.”
Are Your Health Problems Related to Artificial Sweeteners?
Many people belatedly realize they’ve been suffering reactions to one artificial sweetener or another. If you suspect an artificial sweetener might be to blame for a symptom you’re having, a good way to help you weed out the culprit is to do an elimination challenge. It’s easy to do, but you must read the ingredient labels for everything you put in your mouth to make sure you’re avoiding ALL artificial sweeteners. To determine if you’re having a reaction to artificial sweeteners, take the following steps:
- Eliminate all artificial sweeteners from your diet for two weeks.
- After two weeks of being artificial sweetener-free, reintroduce your artificial sweetener of choice in a significant quantity (about three servings daily). Avoid other artificial sweeteners during this period.
- Do this for one to three days and notice how you feel, especially as compared to when you were consuming no artificial sweeteners.
- If you don’t notice a difference in how you feel after re-introducing your primary artificial sweetener for a few days, it’s a safe bet you’re able to tolerate it acutely, meaning your body doesn’t have an immediate, adverse response. However, this doesn’t mean your health won’t be damaged in the long run.
- If you’ve been consuming more than one type of artificial sweetener, you can repeat steps 2 through 4 with the next one on your list.
Lets make it abundantly clear that even though you may not show immediate signs of any noticeable reaction after consuming artificial sweeteners, please don’t make the mistake of telling yourself “they must be OK for me”. Experts strongly urge you to avoid them at all costs. They are toxic to all humans and will not help you in any way, shape, or form.
Are there ANY Safe and Healthy Alternatives to Sugar?
The best strategy is to lower your use of sugar and eat right for your nutritional type and use the right fuel for your genetics and biochemistry making sure you have enough high quality fats. Once your body has the proper fuel, your sweet cravings will radically diminish and you will be satisfied without them. If you still have cravings it is a strong suggestion you need to further refine your attempt to identify the right fuel for your body. If you need a sweetener you could use stevia or Lo Han, both of which are safe natural sweeteners.
Remember, if you struggle with high blood pressure, high cholesterol, diabetes or extra weight, then you have insulin sensitivity issues and would benefit from avoiding ALL sweeteners. As for sodas and other high sugary content or artificially sweetened… wean yourself off of them and go with water instead.
Could artificial sweetener CAUSE diabetes?
Splenda modifies the way the body handles sugar’, increasing insulin production by 20%
- Study found sugar substitute sucralose had an effect on blood sugar levels
- Also discovered that insulin production increased by 20% when consumed
- Scientists aren’t sure what implications are, but said that regularly elevated insulin levels could eventually cause insulin resistance and even diabetes
Splenda is made of sucralose, which has been found to affect blood glucose and insulin levels. Scientists found that consuming the sugar alternative made of sucralose caused a person’s sugar levels to peak at a higher level and in turn increase the amount of insulin a person produced. Researchers also said that while they did not fully understand the implications of the findings, they might suggest that Splenda could raise the risk of diabetes. This is because regularly elevated insulin levels can lead to insulin resistance, which is a known path to type 2 diabetes.
“Our results indicate that this artificial sweetener is not inert – it does have an effect,” said Yanina Pepino, research assistant professor of medicine at the Washington School of Medicine in St. Louis, who led the study. “And we need to do more studies to determine whether this observation means long-term use could be harmful.”Sucralose is made from sugar, but once processed its chemical make up is very different. Gram for gram it is 600 times sweeter than table sugar.
The scientists analysed the effects of Splenda in 17 severely obese people who did not have diabetes and did not use artificial sweeteners regularly. Participants had an average body mass index of just over 42. A person is considered obese when their BMI reaches 30.
Scientists gave subjects either water or dissolved sucralose to drink before they consumed glucose (sugar). They wanted to understand whether the combination of sucralose and glucose would affect insulin and blood sugar levels. Every participant was tested twice. Those who drank water followed by glucose in one visit drank sucralose followed by glucose in the next. In this way, each person served as his or her own control group.“We wanted to study [overweight people] because these sweeteners frequently are recommended to them as a way to make their diets healthier by limiting calorie intake,” Pepino said.They found that when study participants drank sucralose, their blood sugar peaked at a higher level than when they drank only water before consuming glucose. Insulin levels also rose about 20 percent higher.
So despite no extra sugar being consumed, the artificial sweetener was related to an enhanced blood insulin and glucose response. Professor Yanina explained that they do not fully understand the implications that these rises could have.She said: “The elevated insulin response could be a good thing because it shows the person is able to make enough insulin to deal with spiking glucose levels. But it also might be bad because when people routinely secrete more insulin, they can become resistant to its effects, a path that leads to type 2 diabetes.”
It has been thought that artificial sweeteners, such as sucralose, don’t have an effect on metabolism.
They are used in such small quantities that they don’t increase calorie intake. Rather, the sweeteners react with receptors on the tongue to give people the sensation of tasting something sweet without the calories associated with natural sweeteners, such as table sugar.
But recent findings in animal studies suggest that some sweeteners may be doing more than just making foods and drinks taste sweeter. One finding indicates that the gastrointestinal tract and the pancreas can detect sweet foods and drinks with receptors that are virtually identical to those in the mouth.That causes an increased release of hormones, such as insulin. Some animal studies also have found that when receptors in the gut, are activated by artificial sweeteners, the absorption of glucose also increases. But in real life, people rarely consume a sweetener by itself. They use it in their coffee or on breakfast cereal or when they want to sweeten some other food they are eating or drinking.
Just how sucralose influences glucose and insulin levels in people who are obese is still somewhat of a mystery. “Although we found that sucralose affects the glucose and insulin response to glucose ingestion, we don’t know the mechanism responsible,” said Pepino. “We have shown that sucralose is having an effect. In obese people without diabetes we have shown sucralose is more than just something sweet that you put into your mouth with no other consequences. Further studies are needed to learn more about the mechanism through which sucralose may influence glucose and insulin levels, as well as whether those changes are harmful.” The study was published in the journal Diabetes Care.
In a statement, Splenda said: “Numerous clinical studies in people with Type 1 and Type 2 diabetes and non-diabetic people have shown that Splenda Brand Sweetener (sucralose) does not affect blood glucose levels, insulin, or HbA1c.’FDA and other important safety and regulatory agencies from around the world have concluded that sucralose does not adversely affect glucose control, including in people with diabetes.
It has become increasingly harder for the general population to make sound decisions when there is so much contradiction around what is optimal for human consumption.
As far as sweetening agents go Natural versus Artificial, there are as many questions as there are answers. Studies and debates are as controversial as the products themselves depending on who’s conducting them, funding the studies, how the data is perceived / interpreted and reported.
One thing is for certain, a healthy life style, proper diet and exercise will certainly allow you to partake in everything you enjoy… in moderation. Just know the basic facts on your intakes and how it could be adversely affecting you.
My objective is simply provide you with information, to ensure you make the right choices in life, age well and promote positive well-being – Mentally, Physically and Emotionally.
Please read the many other articles posted on our website and should you be in a position where you can benefit from our services
 Talking about the future can be hard. Such discussion will invoke anxiety in even the most calm of us when we start to think about all the unknowns in our futures and those of our loved ones. These discussions can get even harder when it’s not our future we’re talking about, but rather someone else’s. However, as difficult as it may be, there are some questions that we need to have answers to when it comes to our ageing parents and it is wise to have these conversations sooner rather than later. On that note, here are 7 basic questions that you should include in the “talk” with your ageing parent/s… as soon as you can.
Talking about the future can be hard. Such discussion will invoke anxiety in even the most calm of us when we start to think about all the unknowns in our futures and those of our loved ones. These discussions can get even harder when it’s not our future we’re talking about, but rather someone else’s. However, as difficult as it may be, there are some questions that we need to have answers to when it comes to our ageing parents and it is wise to have these conversations sooner rather than later. On that note, here are 7 basic questions that you should include in the “talk” with your ageing parent/s… as soon as you can. Sometimes there’s a lot of pressure to do things in a “traditional” way when it comes to how we remember our loved ones, but that’s not always what they want. Although funerals/memorials need to reflect both the person that is gone and those who are left behind, having a discussion ahead of time can mean that all sides get their voices heard. When a decision is reached beforehand, our loved ones know their wishes will be respected and those of us left behind can know we’re memorializing our parents in a way that they accept as well. This means no guilt for anyone and that’s a much-needed relief at a time of sorrow.
Sometimes there’s a lot of pressure to do things in a “traditional” way when it comes to how we remember our loved ones, but that’s not always what they want. Although funerals/memorials need to reflect both the person that is gone and those who are left behind, having a discussion ahead of time can mean that all sides get their voices heard. When a decision is reached beforehand, our loved ones know their wishes will be respected and those of us left behind can know we’re memorializing our parents in a way that they accept as well. This means no guilt for anyone and that’s a much-needed relief at a time of sorrow. This article delves into ageist stereotypes dressed-up in the garb of myth that biases perceptions and experiences of being old. The article argues current ”mythmaking” about aging perpetuates that which it intends to dispel: ageism. It considers how traditional myths and folklore explained personal experience, shapes social life, and offers meaning for the unexplainable. The current myths of aging perform these same functions in our culture; however, they are based on half-truths, false knowledge, and stated as ageist stereotypes about that which is known. Recent studies in the cognitive sciences are reviewed to provide insight about the mind’s inherent ability to construct categories, concepts, and stereotypes as it responds to experience. These normal processes need to be better understood, particularly regarding how social stereotypes are constructed. Finally, the article argues that ageist stereotypes when labeled as ”myth” even in the pursuit of the realities of aging, neither educate the public about the opportunities and challenges of aging nor inform social and health practitioners about the aged.
This article delves into ageist stereotypes dressed-up in the garb of myth that biases perceptions and experiences of being old. The article argues current ”mythmaking” about aging perpetuates that which it intends to dispel: ageism. It considers how traditional myths and folklore explained personal experience, shapes social life, and offers meaning for the unexplainable. The current myths of aging perform these same functions in our culture; however, they are based on half-truths, false knowledge, and stated as ageist stereotypes about that which is known. Recent studies in the cognitive sciences are reviewed to provide insight about the mind’s inherent ability to construct categories, concepts, and stereotypes as it responds to experience. These normal processes need to be better understood, particularly regarding how social stereotypes are constructed. Finally, the article argues that ageist stereotypes when labeled as ”myth” even in the pursuit of the realities of aging, neither educate the public about the opportunities and challenges of aging nor inform social and health practitioners about the aged.
 A Summary of Canada’s Aging Population
A Summary of Canada’s Aging Population



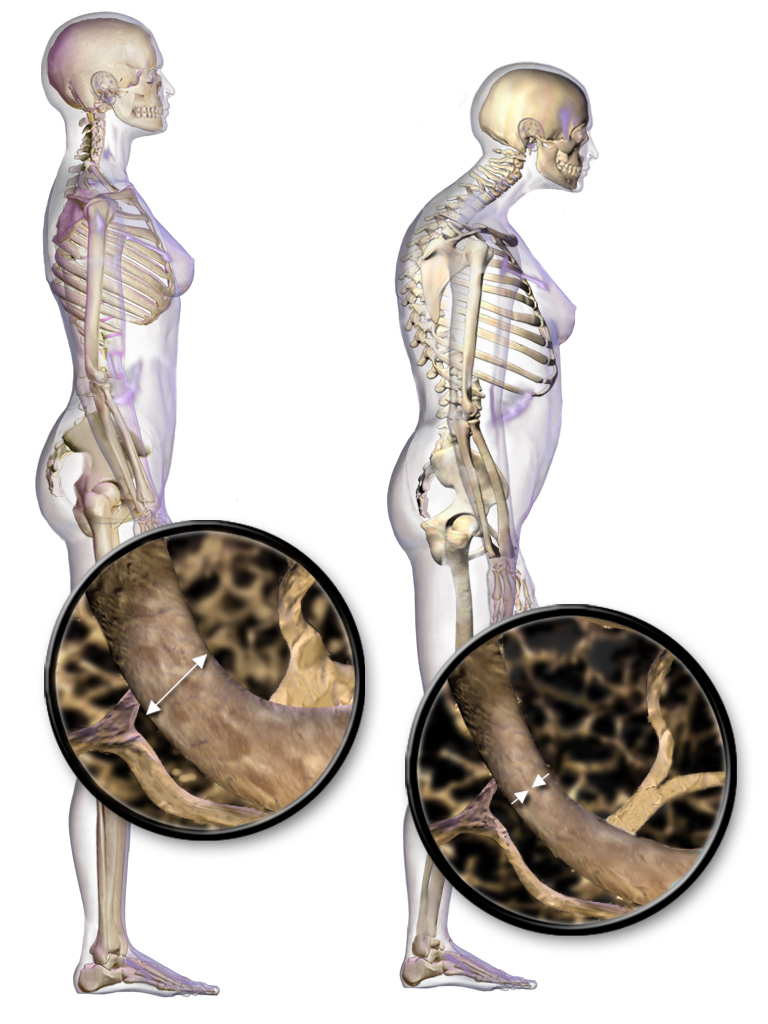 What is Osteoporosis?
What is Osteoporosis?
{kind=link}