Senior Care: Personal & Home Safety

Personal and home safety, for people with alzheimer’s disease and dementia.
Seniors can still remain in their homes, as long as safety measures are put in place to ensure their safety.
As Dementia and Alzheimer’s progresses, a person’s abilities change. But with some creativity and problem solving, you can adapt the home environment to support these changes.
How Dementia affects safety
Alzheimer’s disease causes a number of changes in the brain and body that may affect safety. With creativity and flexibility, you can create a home that is both safe and supportive of the person’s needs for social interaction and meaningful activity.
Depending on the stage of the disease, these can include:
- Judgment: forgetting how to use household appliances
- Sense of time and place: getting lost on one’s own street; being unable to recognize or find familiar areas in the home
- Behavior: becoming easily confused, suspicious or fearful
- Physical ability: having trouble with balance; depending upon a walker or wheelchair to get around
- Senses: experiencing changes in vision, hearing, sensitivity to temperatures or depth perception
Home safety tips
- Assess your home: Look at your home through the eyes of a person with dementia. What objects could injure the person? Identify possible areas of danger. Is it easy to get outside or to other dangerous areas like the kitchen, garage or basement?
- Lock or disguise hazardous areas: Cover doors and locks with a painted mural or cloth. Use “Dutch” (half) doors, swinging doors or folding doors to hide entrances to the kitchen, stairwell, workroom and storage areas.
- Home Safety Checklist: Contact us at “In Or Care – Home Care Services to conduct a safety survey and discuss measures to correct findings. The process is easier than you think and solutions need not be cost prohibitive.
- Be prepared for emergencies: Keep a list of emergency phone numbers and addresses for local police and fire departments, hospitals and poison control helplines.
- Make sure safety devices are in working order: Have working fire extinguishers, smoke detectors and carbon monoxide detectors. Routine inspections, testing and replacing back-up batteries on applicable devices as just as important… Don’t assume because you have then, that they’re functioning as they should.
- Install locks out of sight: Place deadbolts either high or low on exterior doors to make it difficult for the person to wander out of the house. Keep an extra set of keys hidden near the door for easy access. Remove locks in bathrooms or bedrooms so the person cannot get locked inside.
- Keep walkways well-lit: Add extra lights to entries, doorways, stairways, areas between rooms, and bathrooms. Use night-lights in hallways, bedrooms and bathrooms to prevent accidents and reduce disorientation.
- Place medications in a locked drawer or cabinet: To help ensure that medications are taken safely, use a pillbox organizer or keep a daily list and check off each medication as it is taken.
- Remove tripping hazards: Keep floors and other surfaces clutter-free. Remove objects such as magazine racks, coffee tables and floor lamps.
- Watch the temperature of water and food: It may be difficult for the person with dementia to tell the difference between hot and cold. Set water temperature at 120 degrees or less to prevent scalding.
- Support the person’s needs: Try not to create a home that feels too restrictive. The home should encourage independence and social interaction. Clear areas for activities.
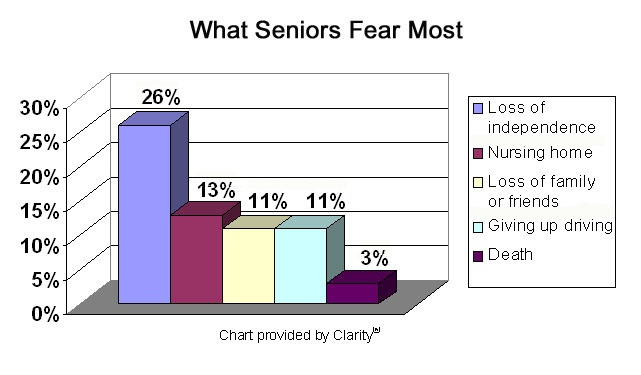
Six in 10 people with dementia will wander
A person with Alzheimer’s may not remember his or her name or address, and can become disoriented, even in familiar places. Wandering among people with dementia is dangerous, but there are strategies and services to help prevent it.
Who is at risk of wandering?
Anyone who has memory problems and is able to walk is at risk for wandering. Even in the early stages of dementia, a person can become disoriented or confused for a period of time. It’s important to plan ahead for this type of situation. Be on the lookout for the following warning signs:
Wandering and getting lost is common among people with dementia and can happen during any stage of the disease.
- Returns from a regular walk or drive later than usual
- Tries to fulfill former obligations, such as going to work
- Tries or wants to “go home,” even when at home
- Is restless, paces or makes repetitive movements
- Has difficulty locating familiar places like the bathroom, bedroom or dining room
- Asks the whereabouts of current or past friends and family
- Acts as if doing a hobby or chore, but nothing gets done (e.g., moves around pots and dirt without actually planting anything)
- Appears lost in a new or changed environment
Tips to prevent wandering
Wandering can happen, even if you are the most diligent of caregivers. Use the following strategies to help lower the chances:
- Identify the most likely times of day that wandering may occur: Plan activities at that time. Activities and exercise can reduce anxiety, agitation and restlessness.
- Reassure the person if he or she feels lost, abandoned or disoriented: If the person with dementia wants to leave to “go home” or “go to work,” use communication focused on exploration and validation. Refrain from correcting the person. For example, “We are staying here tonight. We are safe and I’ll be with you. We can go home in the morning after a good night’s rest.”
- Ensure all basic needs are met: Has the person gone to the bathroom? Is he or she thirsty or hungry?
- Avoid busy places that are confusing and can cause disorientation: This could be shopping malls, grocery stores or other busy venues.
- Place locks out of the line of sight: Install either high or low on exterior doors, and consider placing slide bolts at the top or bottom.
- Camouflage doors and door handles: Camouflage doors by painting them the same color as the walls, or cover them with removable curtains or screens. Cover knobs with cloth the same color as the door or use childproof knobs.
- Use devices that signal when a door or window is opened: This can be as simple as a bell placed above a door or as sophisticated as an electronic home alarm.
- Provide supervision: Never lock the person with dementia in at home alone or leave him or her in a car without supervision.
- Keep car keys out of sight: A person with dementia may drive off and be at risk of potential harm to themselves or others.
- If night wandering is a problem: Make sure the person has restricted fluids two hours before bedtime and has gone to the bathroom just before bed. Also, use night-lights throughout the home.
Make a plan
The stress experienced by families and caregivers when a person with dementia wanders and becomes lost is significant. Have a plan in place beforehand, so you know what to do in case of an emergency.
- Keep a list of people to call on for help: Have telephone numbers easily accessible and update them every six months.
- When someone with dementia is missing: Begin search-and-rescue efforts immediately. Ninety-four percent of people who wander are found within 1.5 miles of where they disappeared.
- Ask neighbors, friends and family to call if they see the person alone.
- Keep a recent, close-up photo and updated medical information on hand to give to police.
- Know your neighborhood: Pinpoint dangerous areas near the home, such as bodies of water, open stairwells, dense foliage, tunnels, bus stops and roads with heavy traffic.
- Keep a list of places where the person may wander: This could include past jobs, former homes, places of worship or a restaurant.
- Provide the person with ID jewelry: Medical alert bracelet and or electronic wander guard device preferably with GPS capability.
- If the person does wander, search the immediate area for no more than 15 minutes: Call “911” and report to the police that a person with Alzheimer’s disease — a “vulnerable adult” — is missing. A Missing Report should be filed and the police will begin to search for the individual. Make a point of knowing what they’re wearing for a more accurate description.
Many people with dementia want to live at home for as long as possible. Often, this is with support from others. However, it can be difficult managing everyday situations if you have dementia, particularly as the dementia progresses and you get older. As a result, some people may not be as safe at home as they used to be. This factsheet looks at how a person with dementia can stay safe at home and in the surrounding environment. It identifies some risks in the home environment and suggests ways to manage them.
It is important to find the right balance between independence and unnecessary harm. The person with dementia should, where possible, be involved in decision-making and their consent sought and given about changes. If this is not possible, it is important that those making the decision do so in the person’s best interests.
Many of the issues in this factsheet are related to the normal ageing process. However, having dementia can place a person at higher risk of experiencing some of these issues. Everyone will experience dementia in their own way. The type of risks they face, and strategies to manage these, will depend on the individual and their situation.
Avoid falls
Falls are a common and potentially serious problem affecting older people. The risk of falls increases with age. This may be because of a range of factors: medical conditions (such as stroke), medication, balance difficulties, visual impairment, cognitive impairment and environmental factors. Falls can have detrimental effects on people, including injuries, loss of confidence and reduced activity.
For some people with dementia, the condition can also increase the likelihood of falling.
There are a number of things that can be done at home to reduce the risk of falling:
- Home safety: Check the home for potential hazards such as rugs, loose carpets, furniture or objects lying on the floor. An occupational therapist may be able to help with identifying hazards and suggesting appropriate modifications.
- Exercise: Regular exercise can improve strength and balance and help to maintain good general health. A referral to a physiotherapist may also help. Speak to your GP to find out more.
- Healthy feet: Foot problems, including foot pain and long toenails, can contribute to an increased risk of falls. Seeing a podiatrist (a health professional who specializes in feet) can help. Contact your doctor to find out more.
- Medicines: Medication can have side effects, including dizziness, which could increase the risk of a fall. Changes to medication or dosage, as well as taking multiple medicines, can increase a person’s risk of falling. Speak to the doctor about a medicine review if the person with dementia is taking more than four medicines.
- Eyesight: Regular eye tests and wearing the correct glasses may help to prevent falls.
- Keep objects in easy reach: If something is going to be used regularly, keep it in a cupboard or drawer that is easy to access.
- Try not to rush: Do things at an appropriate pace; many people fall when they are rushing.
Improve lighting
As people get older they need more light to see clearly. This is because of age-related changes to the eyes. These changes include:
- Pupils becoming smaller
- Increased sensitivity to glare
- Reduced amount of light reaching the retina.
Dementia can cause damage to the visual system (the eyes and the parts of the nervous system that process visual information), and this can lead to difficulties. The type of difficulty will depend on the type of dementia. Problems may include:
- Decreased sensitivity to differences in contrast (including colour contrast such as black and white, and contrast between objects and background)
- Reduced ability to detect movement
- Reduced ability to detect different colours (for example, a person may have problems telling the difference between blue and purple)
- Changes to the visual field (how much someone can see around the edge of their vision while looking straight ahead)
- Double vision.
Improved lighting can reduce falls, depression and sleep disorders, and improve independence and general health. The following tips may help:
- Increase light levels and use daylight where possible.
- Minimize glare, reflection and shadows. Glare can be distracting and can reduce a person’s mobility.
- Lighting should be uniform across any space, and pools of light and sudden changes in light levels should be avoided. This is because when a person gets older, their eyes adapt slowly to changes in light levels.
- Remove visual clutter and distractions such as carpets with floral patterns.
- Use colour contrasts to make things clearer, ie: a light door with a dark frame.
- Leave a light on in the toilet or bathroom during the night. A night-light in the bedroom may help if someone gets up in the night.
Store dangerous substances safely
Dangerous substances, including medicines and household cleaning chemical should be stored somewhere safe. If the person with dementia is unable to administer their own medication safely, arrangements should be made for someone else to do this. A dosette box could be helpful. These have separate tablet compartments for days of the week and/or times of day such as morning, afternoon and evening.
Adaptations to the home
As people get older they may experience difficulties in managing everyday activities such as cooking or bathing, for a variety of reasons. People with dementia may experience additional challenges as their dementia progresses, because of memory problems or a reduced ability to carry out tasks in the correct sequence.
Adapting the home can help people with dementia to maintain their independence and reduce the risk of harm. It can also help to adapt some everyday tasks slightly. The following tips may help:
- Label cupboards and objects with pictures and words so that they can be identified.
- Where possible, use devices that only have one function and are easy to identify, for example a kettle.
- Place clear instructions that can easily be followed somewhere visible.
- Make sure the kitchen is well lit.
- If there are concerns about using gas or electrical appliances inappropriately, contact the gas or electricity company and ask for the person to be put on the priority service register. This means that they will be eligible for free regular safety checks and will be able to get advice about safety measures such as isolation valves (advice is also available for care givers).
- Fit an isolation valve to a gas cooker so that the cooker cannot be turned on and left on. Devices are also available for electric cookers.
- Look into products that may help to maintain independence and safety such as electric kettles that switch off automatically.
- If the person’s ability to recognize danger is declining, consider removing potentially dangerous implements such as sharp knives, but place other items for everyday use within easy reach.
- Create a “wander loop” in your home, a safe pathway that allows the patient to safely roam.
- Use reflector tape to create a path to the bathroom.
- Cover radiators and electrical outlets with guards.
- Lock doors that lead to places like basements and garages.
- Install safety locks and alarms on exit doors and gates.
- Cover smooth or shiny surfaces to reduce confusing glare.
- Eliminate shadows with a lamp that reflects off the ceiling.
- Cover or remove mirrors if they are upsetting to a person with hallucinations.
- Store car keys in a locked container; disable the car.
- Do not allow unattended smoking.
- Make sure an I.D. bracelet is being worn at all times.
- When selecting home care, make sure to hire an aide who has been trained to deal with dementia and Alzheimer’s patients, and is under the supervision of a skilled home care nurse.
- And, most importantly, constantly re-assess your parent’s abilities with the help of a nurse or physician.
Avoid fire
There are ways to minimize the risk of fire in the home, including fitting smoke alarms and carbon monoxide detectors, and checking home appliances.
Local fire and rescue services can provide free home safety visits. They offer advice about how to make the home safer, as well as fitting smoke alarms and planning escape routes. Electric and gas appliances can be dangerous. It is important to check appliances to make sure they are working safely. Some appliances will have built-in safety features. Consider placing safety devices on stoves so that they are not accidently placed, or left on the on position.
Stay safe outdoors
Being outdoors is important for people of all ages and has many benefits. It is good for mental and physical health, including wellbeing, sleep and appetite Being outdoors can have psychological benefits such as reduced depression and agitation. Activity can also enhance a person’s independence and wellbeing. A garden, balcony or outdoor space can help to bring these benefits to people with dementia. It is important to manage any risks that may come with being outdoors.
The Following suggestions may help:
- Make sure the area is well lit. This could be done with a sensor light, so that if a person is outside and daylight is fading they are still able to see adequately.
- Put a rail on any stairs to help the person get up and down them. It can also help to highlight the edges of each step.
- Avoid trip hazards such as loose paving slabs or uneven surfaces.
- Have seating areas so that the person can take a rest or enjoy being outside if they are unsteady on their feet.
- Use shelter to protect people from the elements if they want to spend a long time outside – a parasol or hat to minimize sun exposure.
Ensuring your home is adequately assessed for safety concerns is you first step in assuring that your love one enjoys their decision to remain in their home for as long as possible.
We can help. From an initial assessment to providing the home care services you need to meet your needs.
 died. Over the next few days what will that look like for your loved ones? Your family is grief stricken and they must decide what to do with your body. They love you and want to honor your life. They go to the funeral home to make the arrangements and it is here they learn just how much their ideal tribute to you will cost.
died. Over the next few days what will that look like for your loved ones? Your family is grief stricken and they must decide what to do with your body. They love you and want to honor your life. They go to the funeral home to make the arrangements and it is here they learn just how much their ideal tribute to you will cost. ax advantages associated with an EFA (Eligible Funeral Arrangement). The Federal Government permits any amount to be paid into a prepaid funeral certificate, and the first $15,000 earns tax-exempt interest.
ax advantages associated with an EFA (Eligible Funeral Arrangement). The Federal Government permits any amount to be paid into a prepaid funeral certificate, and the first $15,000 earns tax-exempt interest.
 A Summary of Canada’s Aging Population
A Summary of Canada’s Aging Population